Ankylosing Spondylitis (AS) is a chronic, inflammatory form of arthritis that primarily targets the axial skeleton—specifically the spine and the sacroiliac (SI) joints where the spine meets the pelvis. Unlike common “wear-and-tear” back pain, AS is an autoimmune condition where the body’s immune system mistakenly attacks healthy joint tissue.
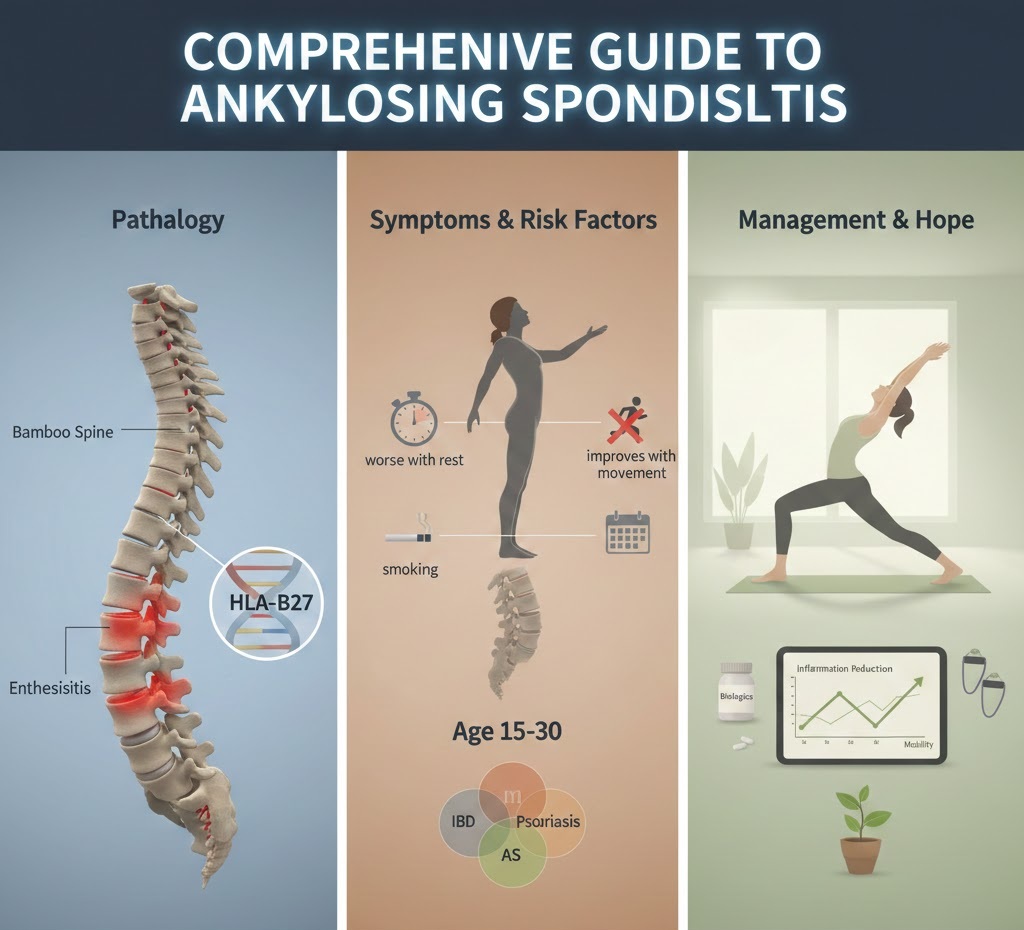
1. Understanding the Pathology: What Happens to the Body?
In a healthy spine, vertebrae are held together by flexible ligaments and tendons. In a person with AS, the body remains in a state of chronic inflammation.
- Enthesitis: This is the hallmark of AS. It is inflammation at the “enthesis”—the site where tendons or ligaments attach to the bone.
- Syndesmophytes: As the body attempts to heal from this inflammation, it produces extra calcium. This leads to the growth of new bone, known as syndesmophytes.
- Fusion (Ankylosis): Over time, these bony growths can bridge the gap between vertebrae, causing them to fuse together. This creates a rigid, inflexible spine often referred to as “Bamboo Spine.”
2. Identifying the Symptoms
AS symptoms usually appear in waves called “flares,” followed by periods of remission.
- Inflammatory Back Pain: Pain is typically worse in the morning or after periods of inactivity. Crucially, it improves with movement and exercise, which is the opposite of mechanical back strain.
- Reduced Chest Expansion: If the inflammation affects the joints where the ribs attach to the spine, it can become difficult to take deep breaths.
- Systemic Involvement: * Uveitis: Redness, pain, and light sensitivity in the eyes.
- Fatigue: A heavy, crushing tiredness caused by the body constantly fighting inflammation.
- Peripheral Arthritis: Pain in large joints like the hips, knees, or shoulders.
3. Risk Factors and Triggers
- Genetics (HLA-B27): The majority of people with AS carry the HLA-B27 gene. While carrying the gene doesn’t guarantee you will develop AS, it significantly increases susceptibility.
- Age and Gender: Symptoms typically emerge between ages 15 and 30 and are rarely diagnosed after age 45. Historically, it was thought to be a “male disease,” but it is now known that women also develop AS, though their symptoms may present differently (often affecting the neck rather than the lower back).
- Associated Conditions: There is a high overlap with Inflammatory Bowel Disease (IBD), such as Crohn’s or Ulcerative Colitis, and the skin condition Psoriasis.
4. Diagnosis and Clinical Tests
Because back pain is so common, AS is often misdiagnosed for years. Rheumatologists use a combination of:
- Imaging: X-rays can show advanced fusion, but MRI is the “gold standard” for catching early-stage inflammation before permanent bone damage occurs.
- Blood Work: Tests for C-Reactive Protein (CRP) and Erythrocyte Sedimentation Rate (ESR) check for general inflammation levels.
- Physical Exam: The “Schober’s Test” measures how much the lumbar spine flexes when the patient bends forward.
5. Treatment and Long-Term Management
While there is no cure, modern medicine aims to stop the progression of fusion and maintain a straight posture.
- Biologics and Biosimilars: Medications like TNF inhibitors or IL-17 inhibitors block the specific proteins that trigger inflammation.
- Physical Therapy: This is non-negotiable. Specialized exercises focus on “extension” (stretching backward) to prevent the spine from fusing in a hunched-forward position.
- Lifestyle Modifications:
- Smoking Cessation: Smoking accelerates spinal fusion and reduces lung function, making AS symptoms significantly worse.
- Sleep Surface: Using a firm mattress and a thin pillow can help keep the spine straight during the night.