Chronic Myeloid Leukemia (CML) is a slow-growing cancer that begins in the bone marrow. It is characterized by the overproduction of a specific type of white blood cell called granulocytes. While these cells are supposed to protect the body, in CML they are abnormal and multiply out of control, eventually “crowding out” healthy red blood cells and platelets.
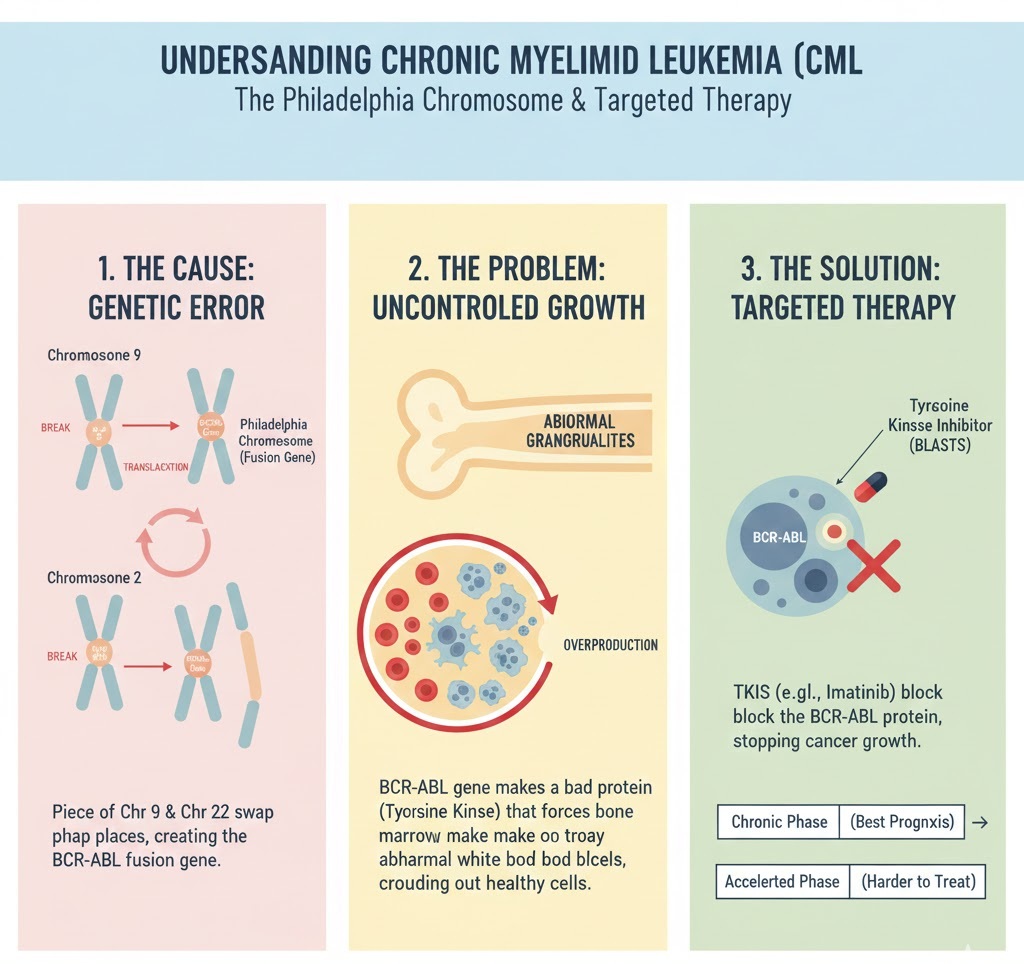
1. The Cause: The Philadelphia Chromosome
Unlike many cancers, CML has a very specific genetic “switch.” Most patients (about 90–95%) have what is known as the Philadelphia chromosome.
- How it happens: A piece of chromosome 9 and a piece of chromosome 22 break off and trade places.
- The Result: This swap creates a fusion gene called BCR-ABL.
- The Impact: This gene produces an abnormal protein (tyrosine kinase) that acts like a “stuck” gas pedal, telling the bone marrow to keep producing abnormal white blood cells indefinitely.
2. The Three Phases of CML
CML is categorized by the percentage of blasts (immature leukemia cells) found in the blood or bone marrow.
- Chronic Phase: Less than 10% blasts. Most people are diagnosed here and respond well to standard oral medications.
- Accelerated Phase: 10% to 19% blasts. Symptoms like fever and weight loss become more noticeable, and the disease becomes harder to control.
- Blastic Phase (Blast Crisis): 20% or more blasts. The cancer behaves more like an aggressive acute leukemia and may spread to other organs.
3. Diagnosis & Symptoms
Because CML grows slowly, it often has no symptoms in the early stages and is frequently discovered during routine blood work.
- Common Symptoms: Extreme fatigue, night sweats, and a feeling of “fullness” on the left side (due to an enlarged spleen).
- Diagnostic Tests:
- CBC with Differential: To count the number of different blood cells.
- Bone Marrow Aspiration: To examine the cells where they are born.
- FISH or PCR Testing: Specialized genetic tests used to identify the BCR-ABL gene or the Philadelphia chromosome.
4. Treatment: Targeted Therapy
The development of Tyrosine Kinase Inhibitors (TKIs) revolutionized CML treatment.
- Targeted Therapy: Drugs like Imatinib (Gleevec) specifically target the BCR-ABL protein. Instead of killing all fast-growing cells (like traditional chemotherapy), they turn off the specific signal that causes CML cells to grow.
- Stem Cell Transplant: Generally reserved for younger patients or those who do not respond to TKIs, as it is a more intensive “reset” of the bone marrow.
- Splenectomy: In rare cases, the spleen is surgically removed if it becomes painfully large and doesn’t respond to other treatments.