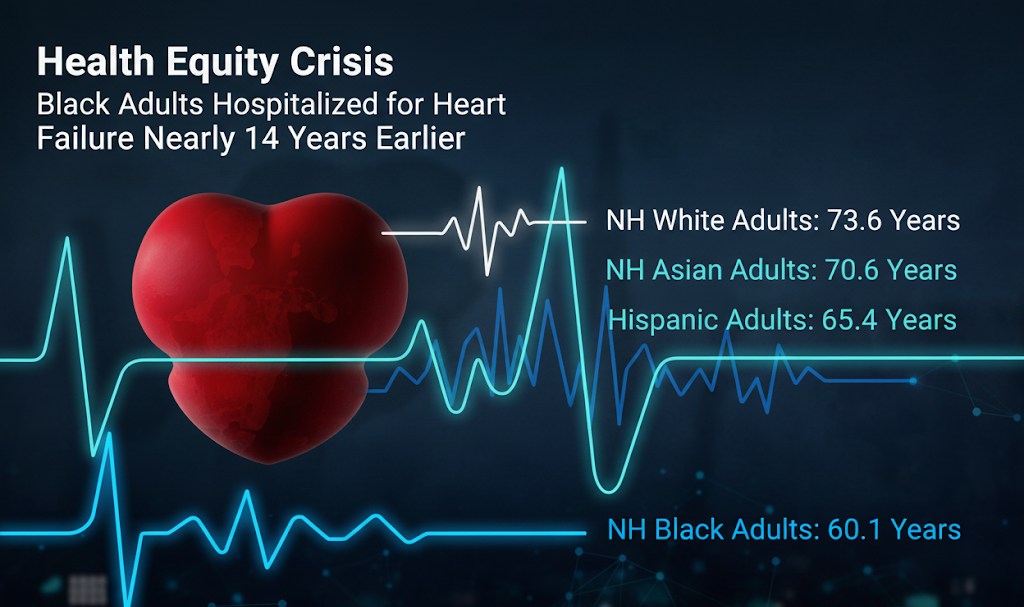
Health Equity Crisis: Black Adults Hospitalized for Heart Failure Nearly 14 Years Earlier Than White Counterparts
A groundbreaking study by Northwestern Medicine investigators, published in the Journal of the American College of Cardiology, has uncovered a severe health equity crisis: Black adults in the U.S. are first hospitalized for heart failure (HF) nearly 14 years earlier than White adults. Significant disparities were also observed in Hispanic and Asian populations, highlighting a systemic issue in cardiovascular health.
This extensive analysis, which examined over 40,000 hospitalized patients across the nation, directly links these alarming disparities to crucial socioeconomic factors, including disparities in insurance coverage and educational levels within communities.
The Disproportionate Burden of Heart Failure
Heart failure is a leading cause of death globally, and its impact is projected to grow. However, its burden is far from evenly distributed. Underrepresented racial and ethnic groups consistently face higher incidence and significantly earlier onset of HF. This aligns with existing research indicating that geographical factors, such as residence in Southern states, rural areas, and economically deprived communities, also correlate with higher HF mortality.
To gain a clearer understanding of these age-related disparities, investigators utilized the Get With the Guidelines—Heart Failure (GWTG-HF, 2016–2019) registry. Their goal was to pinpoint the age of first HF hospitalization across various racial and ethnic groups and identify the associated social risk factors contributing to these differences. Such insights are crucial for policymakers and healthcare providers to develop targeted solutions.
A Decade-Plus Difference in HF Onset
The study meticulously analyzed 42,252 patients with no prior HF diagnosis who experienced their first captured HF hospitalization. The racial/ethnic breakdown included 2% non-Hispanic (NH) Asian, 24% NH Black, 7% Hispanic, and 67% NH White adults.
The findings were unequivocal:
- NH Black patients experienced their first HF hospitalization at an average age of 60.1 years.
- Hispanic patients at 65.4 years.
- NH Asian patients at 70.6 years.
- In stark contrast, NH White patients were first hospitalized at an average age of 73.6 years.
- This represents a difference of 13.5 years for NH Black patients and 8.2 years for Hispanic patients compared to NH White patients.
Variations in clinical and social risk factors were significantly associated with these younger ages at first HF hospitalization across all minority groups, accounting for substantial portions of the age gap. Xiaoning Huang, MD, the study’s first author, emphasized that “social risk factors, including insurance status and area-level educational and economic opportunities, played a major role. These factors often limit people’s access to quality health care and shape people’s health long before they develop heart problems.”
Strategies for Achieving Health Equity in Heart Failure
Addressing these profound disparities requires a multi-faceted approach involving both medical interventions and systemic policy changes:
- Increase Healthcare Capacity: Expanding access to medical treatment, particularly by establishing more healthcare facilities and cardiology services in underserved areas.
- Policy Advocacy: Promoting policies that ensure equal access to economic and educational opportunities, healthy food options, and affordable, high-quality healthcare.
- Early Screening and Prevention: Healthcare systems and pharmacists must be acutely aware of the earlier HF onset in marginalized communities. This necessitates prioritizing heart screenings and delivering thorough patient counseling on preventive strategies, such as smoking cessation, regular exercise, and healthy eating, from an earlier age.
- Building Trust: Given the historical context of medical distrust and exploitation within racial and ethnic minority groups, healthcare professionals, including pharmacists, must actively work to build trustworthy relationships with their patients.
- Connecting Resources: Pharmacists are ideally positioned to connect at-risk patients with essential resources that address both medical and social needs, recognizing the increasingly intertwined nature of these factors in HF management.
Closing these gaps is not merely a medical imperative but a fundamental matter of social justice, requiring concerted efforts to create equitable health outcomes for all.