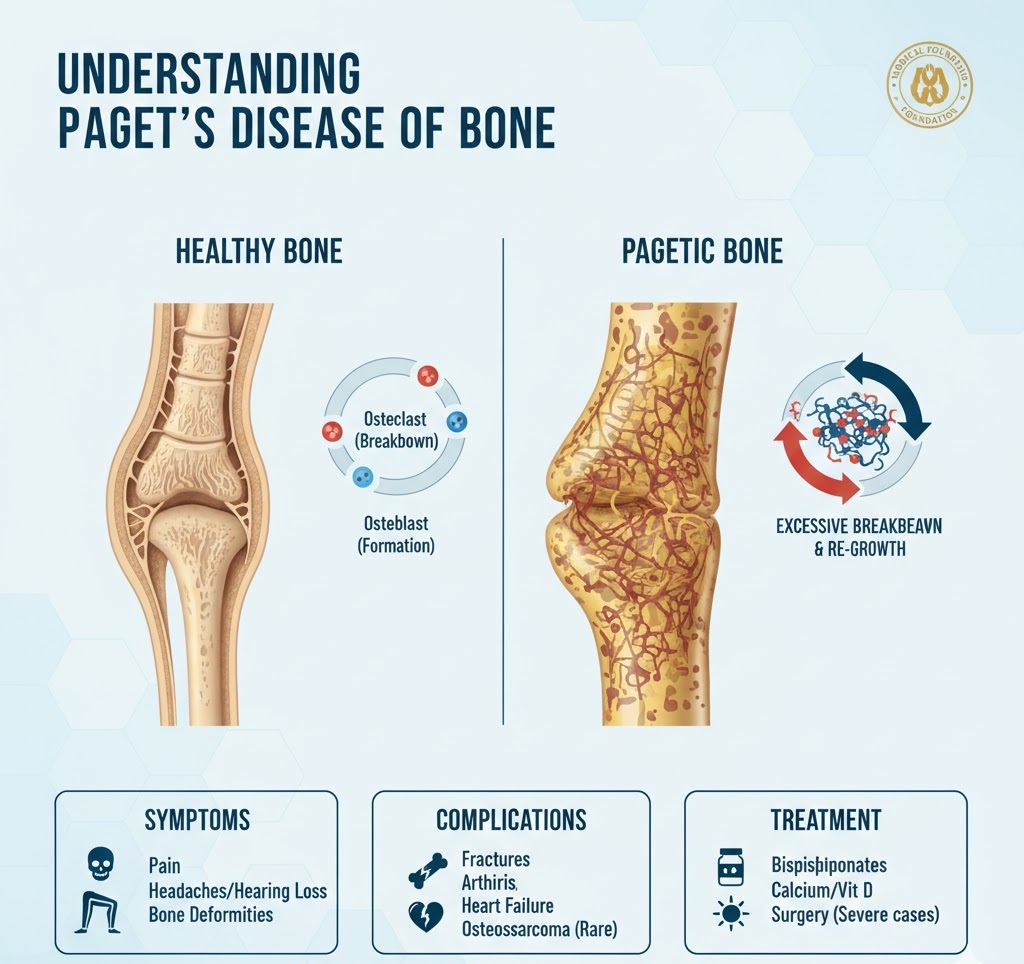
Paget’s disease of bone is a chronic condition that disrupts the body’s normal bone recycling process, where old bone tissue is gradually replaced with new bone tissue. Over time, the affected bones can become fragile, misshapen, and enlarged.
The Pathophysiology of Bone Remodeling
Normally, cells called osteoclasts break down old bone, and osteoblasts build new bone in a balanced cycle. In Paget’s disease, osteoclasts are more active than normal, causing the osteoblasts to respond by working rapidly. This results in bone that is built too fast, leading to a structure that is disorganized, weaker, and larger than healthy bone.
Symptoms and Complications
While many individuals are asymptomatic, those who do experience symptoms may notice:
- Bone Deformities: Most commonly seen as a “bowing” of the legs or an enlarged skull.
- Pain: Dull, aching pain in the bones or joints, often worsening at night.
- Neurological Issues: If the skull or spine is affected, it can compress nerves, leading to hearing loss, headaches, or tingling in the limbs.
Potential Complications
- Fractures and Deformities: Bones break more easily and may heal in curved positions.
- Osteoarthritis: Resulting from the added stress of misshapen bones on nearby joints.
- Heart Failure: In severe cases, the heart must work harder to pump blood to the overactive bone areas.
- Bone Cancer: A very rare complication (less than 1%) known as osteosarcoma.
Diagnosis and Management
Diagnostic Tools
- X-rays: The primary method; shows bone enlargement and characteristic “cotton wool” appearances in the skull.
- Alkaline Phosphatase (ALP) Test: A blood test that measures bone turnover.
- Bone Scan: Uses a radioactive tracer to identify “hot spots” of high bone activity throughout the skeleton.
Treatment Options
The goal of treatment is to reduce bone turnover and prevent complications.
- Bisphosphonates: The most common medication (e.g., Zoledronic acid or Alendronate) to regulate bone building.
- Supportive Care: Adequate intake of Calcium and Vitamin D is essential to support the new bone formation.
- Surgery: Necessary if fractures occur, joints are severely damaged, or nerves are being pinched.
Risk Factors
- Age: Usually diagnosed in people over age 50.
- Ancestry: More common in people of Anglo-Saxon or Northern European descent.
- Family History: Genes like SQSTM1 have been linked to the disorder.