Knee replacement surgery, or knee arthroplasty, is a surgical procedure to resurface a knee damaged by arthritis or injury. Metal and plastic parts are used to cap the ends of the bones that form the knee joint, along with the kneecap, to allow for smooth, pain-free movement.
1. Why Knee Replacement is Performed
The primary goal is to relieve debilitating pain that hasn’t responded to conservative treatments (like injections or physical therapy).
- Osteoarthritis: The “wear-and-tear” type of arthritis that destroys joint cartilage.
- Rheumatoid Arthritis: Chronic inflammation that damages the cartilage and surrounding bone.
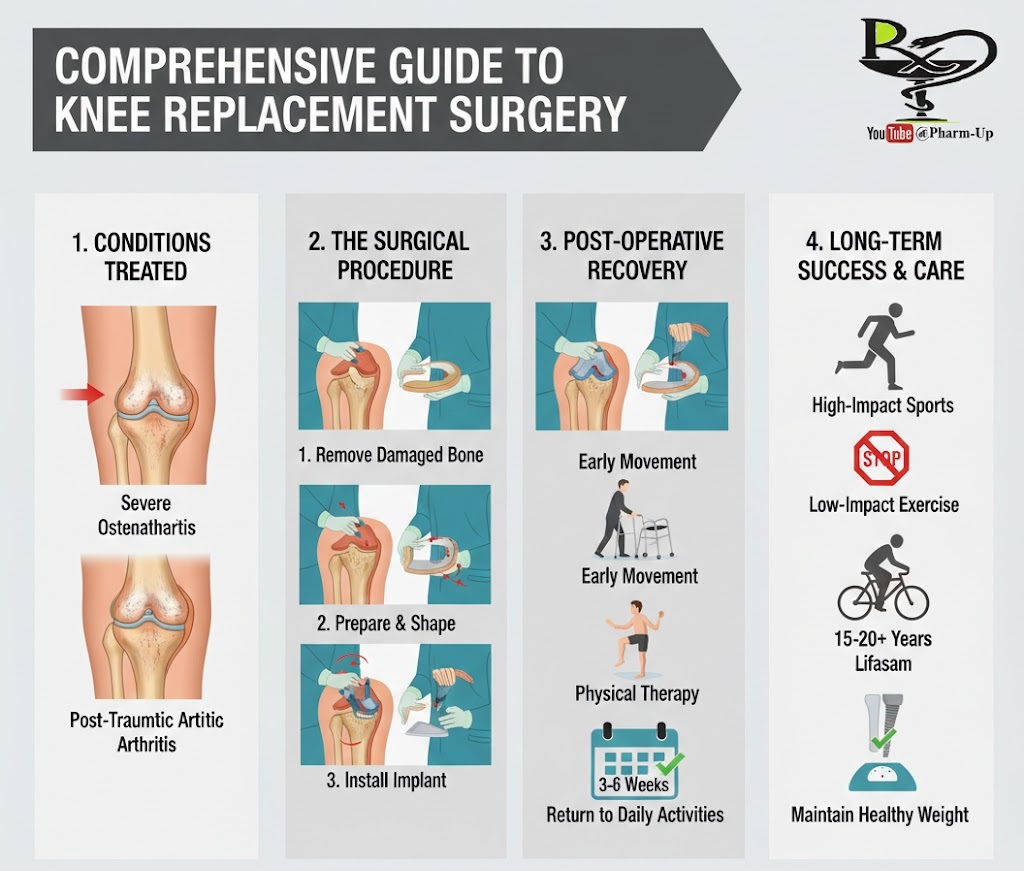
- Post-Traumatic Arthritis: Follows a serious knee injury, such as a fracture or ligament tear, which damages the joint surface over time.
2. Total vs. Partial Knee Replacement
Depending on the extent of the damage, a surgeon may recommend:
- Total Knee Replacement (TKR): The surgeon replaces the surfaces of the thighbone (femur), the shinbone (tibia), and usually the back of the kneecap (patella).
- Partial Knee Replacement: If the damage is limited to only one “compartment” of the knee, only that specific portion is resurfaced, preserving more healthy bone and ligaments.
3. The Surgical Process
- Preparation: The surgeon removes the damaged cartilage and a small amount of underlying bone to create a clean surface.
- Implant Placement: Metal components are typically cemented or “press-fit” onto the bone.
- Resurfacing the Patella: The undersurface of the kneecap is cut and resurfaced with a plastic button (optional depending on the case).
- Insertion of Spacer: A medical-grade plastic spacer is inserted between the metal components to create a smooth gliding surface.
4. Post-Operative Recovery: The Path to Mobility
Recovery is a partnership between the surgeon and the patient.
- The First 24 Hours: Most patients begin standing and taking small steps with a walker the very same day.
- Physical Therapy (PT): This is the most critical factor for success. PT focuses on strengthening the quadriceps and increasing the “flexion” (bend) of the new joint.
- Timeline: Most patients return to light daily activities and driving within 3 to 6 weeks.
5. Long-Term Success and Protection
A modern knee implant typically lasts 15 to 20 years. To maximize its lifespan:
- Avoid High Impact: Avoid running, jumping, or high-intensity sports that put excessive stress on the plastic spacer.
- Low Impact is Key: Walking, swimming, golf, and cycling are excellent ways to stay active without damaging the implant.
- Weight Management: Every extra pound of body weight puts significantly more pressure on the prosthetic joint.