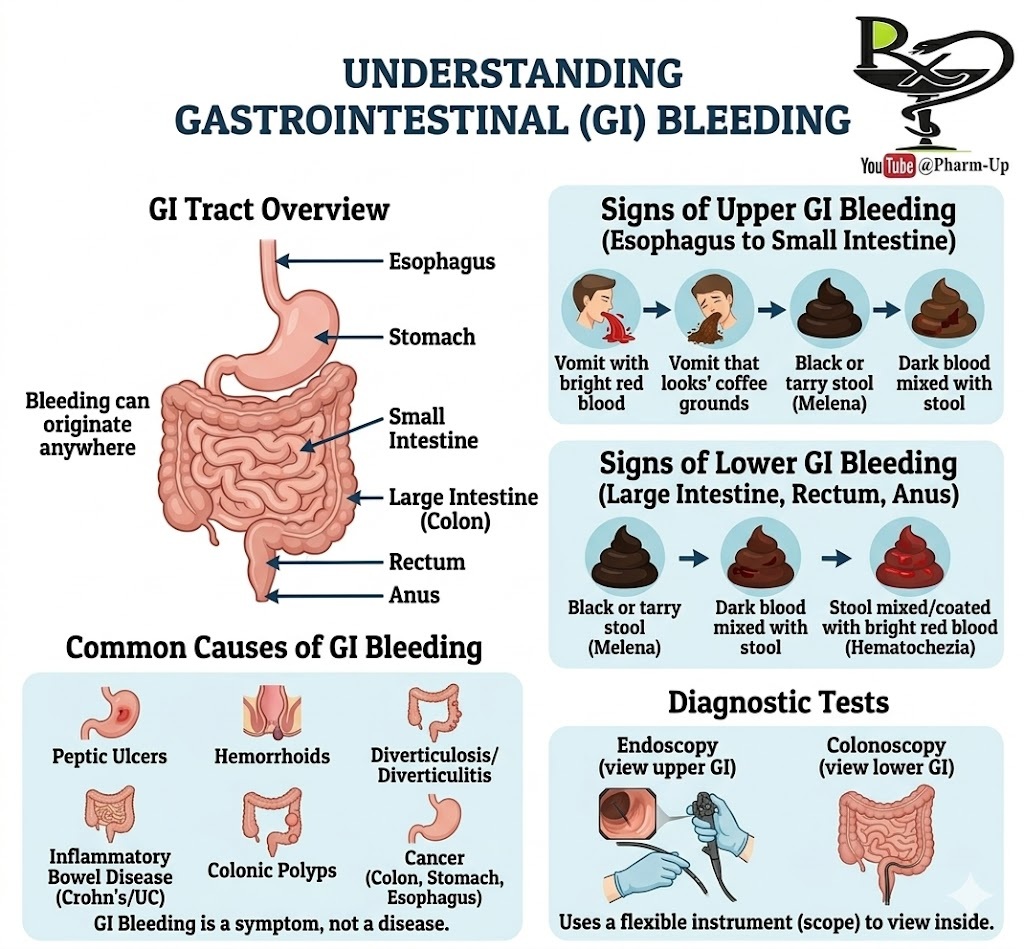
Gastrointestinal (GI) bleeding is a clinical symptom rather than a standalone disease. It indicates an underlying issue somewhere along the digestive tract, which spans from the esophagus down to the anus. The severity can range from microscopic amounts detectable only through laboratory testing (occult bleeding) to heavy, acute episodes.
Identifying the Source: Upper vs. Lower GI Bleeding
The appearance of blood is often the primary clue for doctors to determine the location of the hemorrhage.
- Upper GI Tract (Esophagus, Stomach, Small Intestine):
- Hematemesis: Bright red blood in vomit.
- “Coffee Ground” Vomit: Blood that has been partially digested by stomach acid.
- Melena: Black, tarry, and foul-smelling stools.
- Lower GI Tract (Colon, Rectum, Anus):
- Hematochezia: Bright red blood either mixed with or coating the stool.
- Dark/Maroon Stools: Can occur if the bleeding source is in the upper colon.
Common Causes
Because GI bleeding is a symptom, diagnostic efforts focus on finding the “why.” Common triggers include:
- Inflammatory Issues: Gastritis, esophagitis, Ulcerative Colitis, and Crohn’s disease.
- Structural Abnormalities: Hemorrhoids, anal fissures, diverticulosis, or colonic polyps.
- Ulcers and Tears: Peptic ulcers (often caused by H. pylori or NSAIDs) or Mallory-Weiss tears in the esophagus.
- Malignancy: Tumors or cancer in the esophagus, stomach, or colon.
Diagnosis through Endoscopy
The most effective way to locate and often treat the source of bleeding is through endoscopy.
- Upper Endoscopy (EGD): A flexible scope is inserted through the mouth to examine the esophagus, stomach, and duodenum.
- Colonoscopy: The scope is inserted through the rectum to examine the entire length of the large intestine (colon).