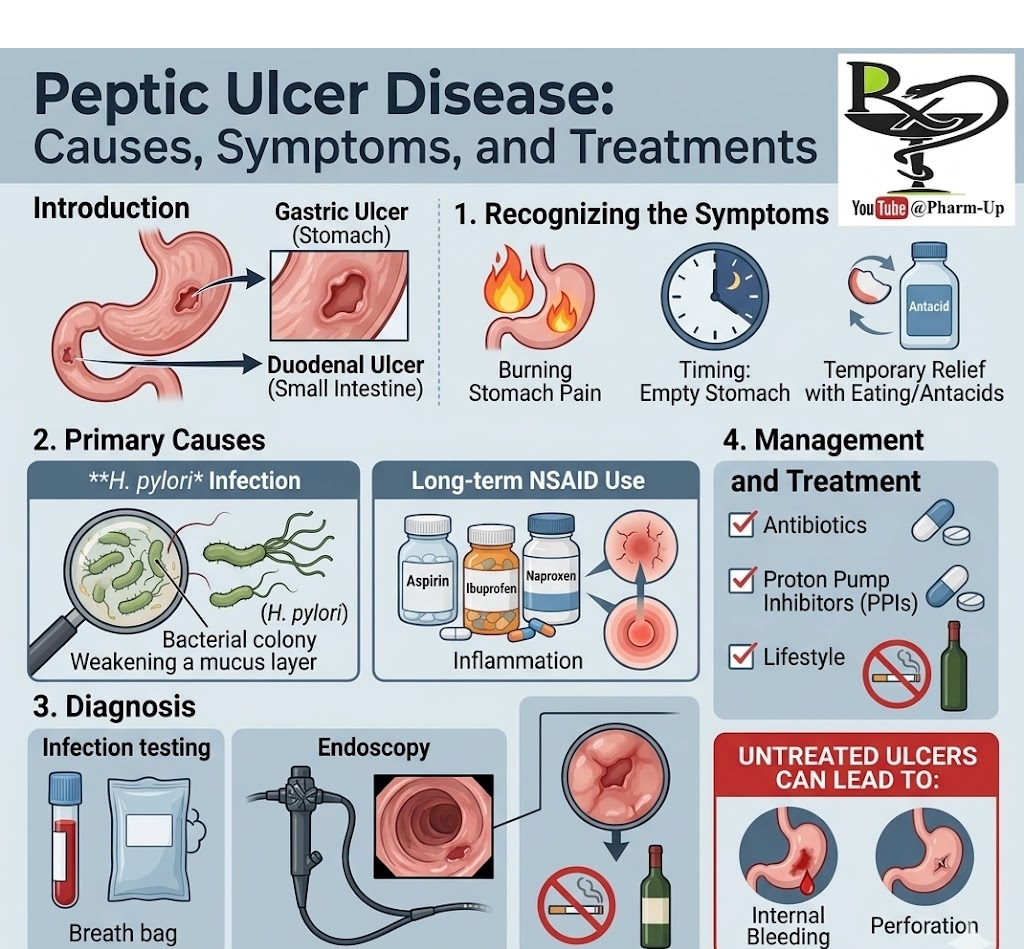
A peptic ulcer is an open sore that develops on the inner lining of your stomach (gastric ulcer) or the upper portion of your small intestine (duodenal ulcer). While often associated with lifestyle, the most common drivers are biological and pharmacological.
Recognizing the Symptoms
The most hallmark sign is a burning sensation in the abdomen, caused by stomach acid coming into contact with the raw ulcerated tissue.
- Timing: Pain typically strikes when the stomach is empty—between meals or in the middle of the night.
- Duration: Discomfort can last from a few minutes to several hours.
- Temporary Relief: Eating or taking antacids may briefly buffer the acid and soothe the pain, but the relief is short-lived as the underlying sore remains.
Primary Causes: Debunking the Myths
For decades, it was believed that stress and spicy food caused ulcers. We now know they are merely triggers that aggravate symptoms, not the root cause.
| Primary Causes | Description |
| H. pylori Infection | A common bacterium that infects the stomach lining, weakening the protective mucus layer. |
| Long-term NSAID Use | Regular use of pain relievers like aspirin, ibuprofen (Advil/Motrin), and naproxen (Aleve) can irritate or inflame the lining. |
Diagnosis and Management
If left untreated, peptic ulcers can lead to internal bleeding or a perforation (hole) in the stomach wall.
Diagnostic Methods
- Infection Testing: Doctors use blood, breath, or stool tests to detect the presence of H. pylori.
- Endoscopy: A small camera is threaded down the throat to provide a direct view of the stomach and duodenum.
Treatment Pathways
- Antibiotics: If H. pylori is detected, a course of antibiotics is required to eradicate the bacteria.
- Proton Pump Inhibitors (PPIs): Medications that block acid production to allow the tissue time to heal.
- Lifestyle Adjustments: Avoiding alcohol and smoking is crucial, as both can interfere with the healing process and increase acid production.