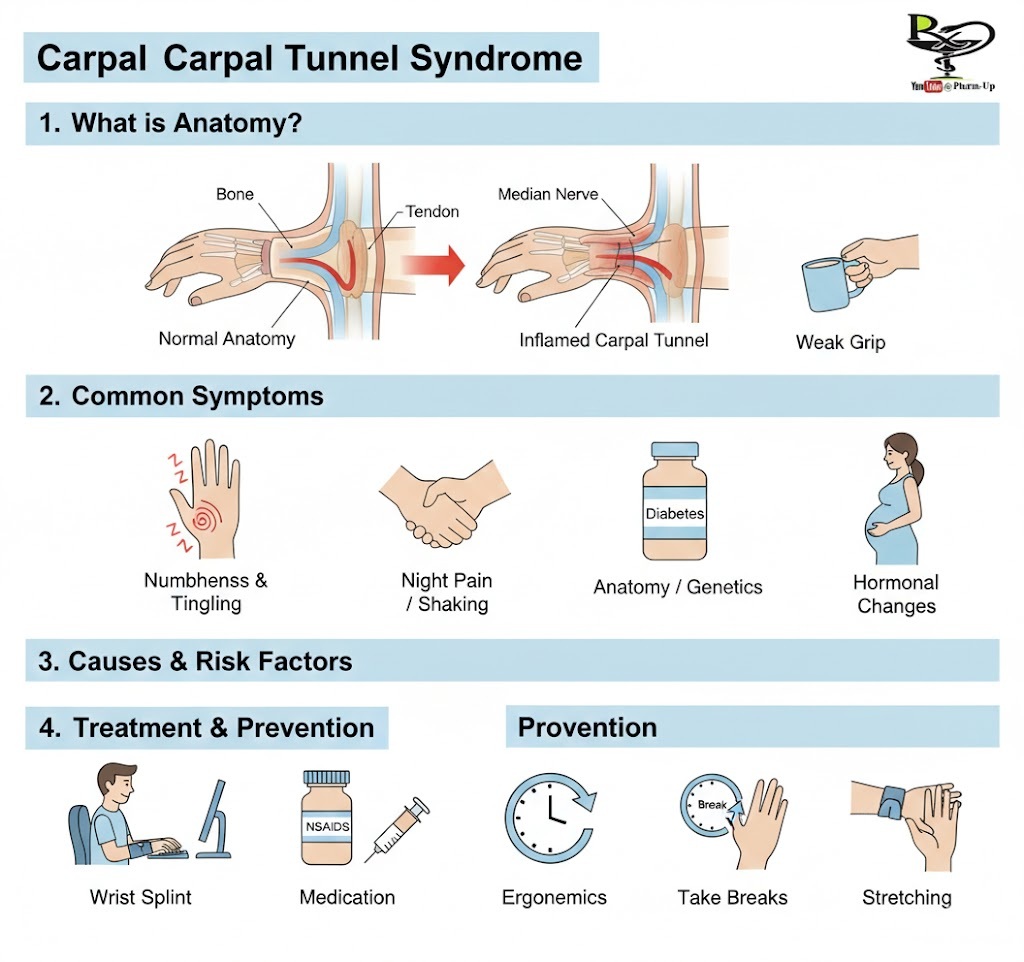
Carpal Tunnel Syndrome (CTS) occurs when the median nerve, which runs from the forearm into the palm of the hand, becomes pressed or squeezed at the wrist. The “carpal tunnel” is a narrow, rigid passageway of ligament and bones at the base of the hand. Because this tunnel is so narrow, any swelling of the tendons or inflammation can pinch the nerve, leading to pain and dysfunction.
1. The Mechanics of the Injury
To understand CTS, it helps to look at the “traffic” inside the wrist:
- The Median Nerve: Controls sensations to the palm side of the thumb and fingers (except the little finger) and sends signals to move the muscles around the base of the thumb.
- The Tendons: Nine tendons that allow the fingers to flex and curl.
- The Squeeze: When the lining of the tendons (synovium) swells, the space inside the tunnel shrinks, putting direct pressure on the median nerve.
2. Recognizing the Symptoms
Symptoms typically begin gradually and are often most noticeable at night.
- Sensory Changes: Frequent burning, tingling, or itching numbness in the palm of the hand and the fingers (especially the thumb, index, and middle fingers).
- The “Hand Shake” Sign: Many people feel the need to “shake out” their hands or wrists to regain feeling.
- Physical Weakness: As the condition progresses, you may experience a decreased grip strength, making it difficult to form a fist, grasp small objects, or perform manual tasks like buttoning a shirt.
3. Common Causes and Risk Factors
CTS is rarely caused by a single factor; it is usually a combination of:
- Anatomy: Smaller carpal tunnels (often hereditary) or wrist fractures that alter the space.
- Gender: Women are at higher risk, possibly due to smaller carpal tunnels or hormonal changes during pregnancy and menopause.
- Chronic Illness: Diabetes and rheumatoid arthritis can cause nerve damage or inflammation.
- Workplace Factors: Repetitive motions, especially those involving vibration or extreme wrist extension/flexion, can increase pressure.
4. Diagnosis and Treatment
Early diagnosis is key to avoiding permanent nerve damage. Doctors use physical tests like Tinel’s Sign (tapping the nerve) or Phalen’s Maneuver (flexing the wrist) to see if symptoms are triggered.
| Treatment Level | Common Methods |
| Non-Surgical | Splinting: Keeping the wrist neutral at night. NSAIDs: Reducing pain/inflammation. Corticosteroids: Injections to reduce swelling. |
| Therapeutic | Yoga & Stretching: To improve flexibility. Ergonomic Adjustments: Modifying workstations. |
| Surgical | Carpal Tunnel Release: Cutting the ligament that forms the roof of the tunnel to relieve pressure on the nerve. |
5. Prevention: Protecting Your Wrists
- Relax Your Grip: If you write or use a keyboard, try to use the least amount of force necessary.
- Neutral Wrist Position: Avoid bending your wrist all the way up or down. A relaxed, middle position is best.
- Take Frequent Breaks: Gently stretch and bend hands and wrists periodically.